The Manual
Tender Point Survey
by David Sinclair, MD,
Terence W Starz, MD, Dennis C Turk, PhD (Jointly sponsored with the
University of Pittsburgh School of Medicine Center For Continuing Education in
the Health Sciences.)
Introduction
Widespread
musculoskeletal pain has long plagued humankind. It made its appearance in past
epochs as lumbago, muscular rheumatism, and fibrositis. Most recently the
condition has been labeled as fibromyalgia (FM).
Although etiology and
pathophysiology of FM are widely debated, the clinical entity described as FM is
estimated to affect from three to six million people in the United States.
Historically, there has been great variability in the criteria used for
diagnosing FM. The American College of Rheumatology (ACR) conducted a
multicenter study published in 1990 that specified two primary criteria that
characterized FM: (1) three or more months of widespread pain defined as pain
present above and below the waist on the right and left side of the body and
along the midline and (2) report of pain at a minimum of 11/18 specified
locations (tender points - TPs) throughout the body when palpated with 4
kilograms of digital pressure. These two criteria were selected from a number of
variables examined as they were shown to reliably discriminate FM from other
musculoskeletal disorders in the multicenter study.
TPs are widely
distributed throughout the musculoskeletal system. They are typically located in
the muscle bodies, over tendinous insertions and at bony prominences. The
anatomic and physiological mechanisms accounting for the presence of TPs have
received great attention but explanation for their origin remains unclear.
A number of factors may
influence the sensitivity of TPs during an examination: (1) the amount of force
applied at the survey site, (2) the number of times (single versus repeated) and
method (finger pad, dolorimeter) by which the force is applied, (3) the
patient's position, which affects muscle tone and survey site localization. The
sequence of site examination may influence the patient's response based on the
anchoring effect of sensations experienced at prior survey sites. A standardized
examination procedure enhances the reliability of survey site reporting,
interobserver reproducibility, the comparability of research studies and the
direction of treatment modalities.
The Manual Tender Point
Survey (MTPS) outlined in this document describes a technique requiring
approximately 5-10 minutes to perform. It is based on the 1990 American College
of Rheumatology tender point protocol for FM. This guide will (1) describe the
pressure application technique, (2) discuss the precise identification of survey
sites, and (3) review the complete Manual Tender Point Survey examination
including the standardized examination procedure and patient instructions.
Pressure
Application Techniques
 The
standard procedure for applying pressure in the Manual Tender Point Survey (MTPS)
uses the thumb pad of the examiner's dominant hand. This method was adopted
because it has been shown to be as reliable as the use of a dolorimeter (strain
gauge). Also, it allows the examiner to make use of important tactile cues.
The
standard procedure for applying pressure in the Manual Tender Point Survey (MTPS)
uses the thumb pad of the examiner's dominant hand. This method was adopted
because it has been shown to be as reliable as the use of a dolorimeter (strain
gauge). Also, it allows the examiner to make use of important tactile cues.
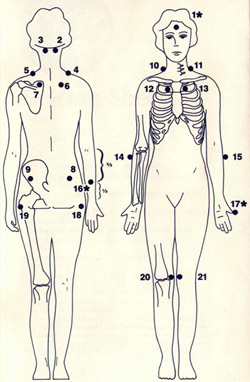
- Survey sites are first
located visually (see figure at right) and then with light palpation.
- Then apply thumb pad
pressure perpendicular to each survey site.
- Each survey is pressed
for a total of 4 seconds only once to avoid sensitization that may
occur with repeated palpation.
- The force is increased
by 1 kg. per second until 4 kg. of pressure is achieved.
- Whitening of the
examiner's nail bed usually occurs when applying the 4 kg. force.
Learning the Feel
of 4 Kilograms
A simple method to learn
the feel of 4 kilograms can be developed by using a standard weight scale.
- The examiner stands
behind the practice subject.
- The scale is first set
at the weight of the subject.
- 4 kg. is then added to
the subject's balanced weight.
- At the trapezius
survey site, enough pressure is applied perpendicularly with the thumb pad
of the dominant hand to return the scale into balance.
- A dolorimeter may also
be used to assist the examiner to acquire the feel of 4 kg of force.
Procedural
Guidelines & Patient Instructions
- The MTPS should be
performed at the beginning of the physical examination because other
examination procedures may sensitize the specified points to the palpation
pressure.
- The patient should
wear a standard gown to permit easy access to palpation sites.
- A scoring
sheet is used to record the results of the examination.
Read
the statement from the scoring sheet:
"Various areas of your body will be examined for pain. Please say 'Yes' or
'No' if there is any pain when I press a specific point."
- If a patient responds,
"Yes" to indicate a site is painful, the examiner should assess
the patient's perception of the pain severity by asking her/him to rate the
pain on a 0 to 10 scale.
Explanation
of the scale is also read to the patient:
"I
want you to rate the intensity of the pain on a scale from 0 to 10. 0 is no pain
and 10 is the worst pain that you have ever experienced." ( After testing
survey site 9, the patient should be reminded of the meaning of the pain scale
to reinforce their understanding of the range.)
The 18 survey sites and 3
control sites are examined in the designated numerical order. The figure above
shows the general location of survey sites.
- Individuals vary in
their judgment of what constitutes a painful sensation. The purpose of the
control sites is to reveal the baseline of the patient's pain perception.
- For survey sites 1-17,
the patient should sit on the end of the exam table.
- Survey sites 18 and 19
are tested with the patient lying on her/his contralateral side from the
site to be tested.
- The patient should lie
on her/his back with feet slightly apart for survey sites 20 and 21.
- Following the testing
at each survey site, the examiner asks the patient, "Is
that painful?" After the response, the examiner will ask
her/him to "Please rate the pain from 0 to
10." The response is immediately recorded on the scoring
sheet where indicated.
- Some patients may have
difficulty following the instructions. When this happens, repeat the
instructions and reassure the patient that "Giving
your best estimate is sufficient." Avoid lengthy discussions
or explanations.
- The Fibromyalgia
Intensity Score is obtained by averaging the scores of the 18 survey sites
(sum of the pain severity ratings divided by 18). The scores of the control
sites may be averaged. These values may be helpful when following patients
through serial examinations over time and to make comparisons among
patients.
Survey Site
Identification
Follow the numerical
sequence:
1. Forehead (Control)
Patient position: Seated,
head in neutral position.
Examiner position: Front
Procedure:
- Support the back of
the head with the examiner's non-
dominant hand.
- Press perpendicularly
to the center of the forehead.
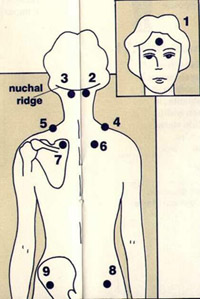 2
& 3. Occiput
2
& 3. Occiput
Patient position: Seated,
head loosely flexed forward approximately thirty degrees
Examiner position: Beside and behind
Procedure:
- Support the head with
the examiner's non-dominant hand on the
forehead.
- Move the examining
thumb up midline of the neck to the nuchal
ridge, then laterally one thumb width in the insertion of the suboccipital
muscles on the occiput.
- Press at this point
just below the nuchal ridge.
4 & 5. Trapezius
Patient position: Seated,
head in neutral position
Examiner position: Beside and behind
Procedure:
- Identify the midpoint
of the upper border of the trapezius.
- Press down.
6 & 7. Supraspinatus
Patient position: Seated
Examiner position: Beside and behind
Procedure:
- Press immediately
above the scapular spine near the medial border of the scapula.
8 & 9. Gluteal
Patient position: Seated
Examiner position: Beside and behind
Procedure:
- Position one hand
loosely on the iliac crest; the thumb falls naturally on the survey site on
gluteus medius, just lateral to gluteus maximus.
- Press perpendicularly
with the examining thumb.
10 & 11. Low Cervical
Patient position: Seated,
head in neutral position
Examiner position: Beside
Procedure:
- Identify the tip of
the mastoid process and cricoid cartilage (C6) below the thyroid cartilage.
- Move the thumb
straight down from the mastoid process to C5-C7 range (cricoid level).
- Support the other side
of the neck.
- Press toward the
opposite shoulder.
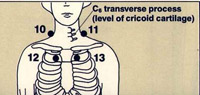 12
& 13. Second Rib
12
& 13. Second Rib
Patient position: Seated
Examiner position: Beside
Procedure:
- Find the sternal
notch; move down to angle of Louis.
- Move to the 1st
palpable rib (2nd rib), one thumb width lateral to manubrium sterni.
- Press the upper
border.
- Support the patient's
back.
14 & 15. Lateral Epicondyle
Patient position: Seated,
hands on lap
Examiner position: Beside
Procedure:
- Support the forearm
with the examiner's non-dominant hand.
- Press over the muscle
2 cm distal to the lateral epicondyle.
 16.
Right Forearm (Control)
16.
Right Forearm (Control)
Patient position: Seated
Examiner position: Beside
Procedure:
- Support the forearm
with the examiner's non-dominant hand.
- Press over the muscle
at junction of distal and middle 1/3 of forearm.
17. Left Thumb (Control)
Patient position: Seated
Examiner position: Beside
Procedure:
- Support the thumb with
the examiner's non-dominant hand.
- Press the entire nail
area of the left thumb.
- Do not squeeze the
thumb between the examiner's thumb and forefinger.
18 & 19. Greater Trochanter
Patient position: Lying
on opposite side, leg loosely flexed at the hip and knee
Examiner position: Beside
Procedure:
- Press perpendicularly
one thumb width posterior to the trochanteric prominence.
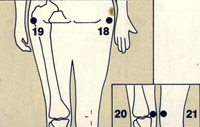 20
& 21. Knee
20
& 21. Knee
Patient position: Lying
on back, feet slightly apart
Examiner position: Beside
Procedure:
- Press just above the
joint line at the medial fat pad.
Review
- The patient should
wear a standard gown for the examination.
- The MTPS instructions
are read to the patient before the examination.
- Survey sites are
examined in numerical order.
- Each survey site is
located first visually and then with light palpation.
- Use the thumb pad of
the dominant hand throughout the examination.
- Thumb pad pressure
should be applied perpendicularly to each survey site..
- Each survey site is
pressed once for a total of 4 seconds.
- The thumb pad force is
increased by 1 kg. per second up to 4 kg.
- The patient responds "Yes"
or "No" if there is any pain after testing each survey
site.
- The patient then rates
the intensity of the pain on a scale from 0 to 10. Do not engage in lengthy
discussions. Ask the patient to, "Give your best estimate."
- The patient's response
to the queries is immediately recorded on a scoring
sheet.
- A Fibromyalgia
Intensity Score is determined by summing the patient's responses on the 0 to
10 scale for each survey site and dividing by 18.
- Patient's baseline
rating of pain is determined by averaging the responses on the 0 to 10 score
for each control site (sites 1, 16 and 17) and dividing by 3.
Variations
Encountered & Their Resolution
Although the standardized
protocol for the Manual Tender Point Survey (MTPS) is designed to increase
reliability, response to physical examination is inherently liable to
variabilities of human perception. Below are listed situations you may encounter
in performing the MTPS. They should not significantly confound the MTPS process.
Quite the contrary the behavioral characteristics should be noted and the
non-verbal communication aspect of the patient's response recognized by the
examiner.
Patients will vary in
their behavior during the MTPS including their response to the pressure
application. Although observing the patient's expressions and body language
enhances the overall assessment, the objectivity of these responses is difficult
to assess reliability. These responses may be recorded along side the individual
survey site scores but are not included in the formal scoring.
On occasion a MTPS may be
confounded to the point of being without value. Abandon the survey at least for
that visit and note the reason.
|
Problem
|
Response
|
| 1. Adipose
tissue obscuring landmarks |
1. Base
survey site location on scoring sheet outline and directions as closely
as possible. |
| 2. Injury
present at survey site area |
2. Note the
finding. |
| 3. Patient
remarks, §Thatïs not where I hurt...¥ |
3. Examiner
responds, §This is not just a search for sore spots. Itïs a survey
of specific locations on your body.¥ |
| 4. Patient
announces response before you complete your pressure application. |
4. Accept
the response and advise the patient to allow the completion of the full
pressure application, if possible. |
| 5. Patient
withdraws before you achieve 4 kg. of pressure. |
5. Accept
this response and record the patientïs numerical score. Note that full
pressure was not applied. |
| 6. Patient
grabs your hand to prevent the pressure application. |
6. Enlist
patient cooperation for maintaining relaxed standardized posture. |
| 7. Assigning
a number for pain may be difficult for a patient. |
7. Remind
her or him of the scale and say, §Giving your best estimate is
sufficient.¥ |
Afterward
It is important to note
that the diagnosis of FM requires both (1) the presence of widespread pain of at
least three months' duration and (2) at least 11/18 positive survey sites. The
presence of 11/18 positive sites alone is not sufficient for the diagnosis of
FM.
The techniques and
guidelines outlined in this booklet are designed to facilitate the following:
- Accurate
identification of the number of painful survey sites
- Determination of a
severity score for each survey site
- Assessment of the
patient's baseline pain perception using control points
- Since it is likely
that performance of the MTPS protocol will drift from the standard over
time, periodic review of these guidelines is recommended.
- Using a standard
weight scale or dolorimeter, the examiner should repeatedly familiarize
himself or herself with the "Feel of 4 Kilograms" at 4 to 5 week
intervals.
- Different procedures
to identify survey sites have been described. The MTPS techniques were
chosen because of their ease of accurate reproducibility. The MTPS is an
assessment of pain at very specific sites; it is not a search for all
areas of musculoskeletal soreness.
The authors are grateful
for the advice and criticism of the many people who contributed to the creation
of this document. For more information on "The Manual Tender Point
Survey" contact:
University of Pittsburgh
Medical Center
Center for Continuing Education in the Health Sciences
522 Nese-Barkan Building
200 Lothrop Street
Pittsburgh, PA 15213
Attn. Linda Levine
Dennis C Turk, PhD
John and Emma Bonica Professor of Anesthesiology and Pain Research
Department of Anesthesiology
University of Washington
Seattle, WA 98195